Articles
Submental Intubation in Maxillofacial Surgery
Submental intubation is a valuable airway management technique in maxillofacial surgery that provides secure airway control while preserving unobstructed access to the oral and nasal cavities. In carefully selected cases, it offers a safe and effective alternative to nasotracheal intubation and tracheostomy.
Why Submental Intubation?
Standard oral or nasotracheal intubation can interfere with surgical access or be contraindicated in patients with facial trauma. Tracheostomy, while effective, carries higher morbidity and long-term complications. Submental intubation bridges this gap by allowing intraoperative airway control without violating the nasal passages or performing a tracheostomy.
Clinical studies have demonstrated that submental intubation is associated with:
-
Low complication rates
-
Minimal scarring
-
Excellent surgical access
-
Rapid reversal at the end of the procedure
Indications
Submental intubation is most commonly indicated when nasotracheal intubation is contraindicated and intraoperative occlusion must be assessed.
Common Indications
-
Contraindications to nasotracheal intubation
-
Epistaxis
-
Cerebrospinal fluid (CSF) leak
-
Rhinorrhea
-
-
Pan-facial trauma
-
Basilar skull fractures
-
Orthognathic surgery combined with rhinoplasty
-
Craniomaxillofacial surgery requiring unobstructed nasal and oral access
Why a Paramedial Submental Incision?
A paramedial approach is preferred over a strict midline incision due to reduced risk to critical anatomic structures.
Advantages of a Paramedial Incision
-
Avoids injury to geniohyoid and genioglossus muscles
-
Avoids the anterior belly of the digastric muscle
-
Avoids the submandibular duct caruncle
-
Reduces risk of postoperative floor-of-mouth complications
Submental Intubation Technique (Paramedial Approach)
Key Pre-Procedure Step
-
Release the endotracheal tube (ETT) connector prior to intubation
-
Use a cuffed, armored (reinforced/anode) endotracheal tube
-
Ensure the T-piece connector can be removed easily
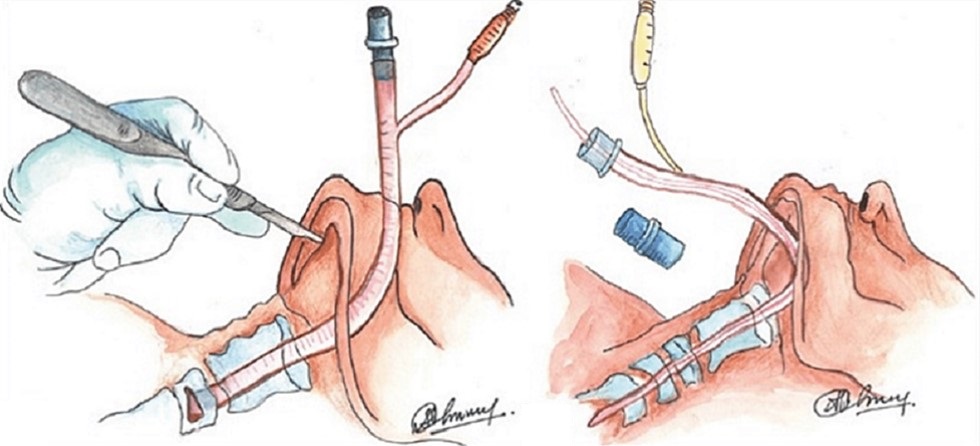
Step-by-Step Procedure
-
Oral Intubation
-
Perform standard oral intubation with a cuffed, metallic coiled (armored) ETT
-
-
Skin Incision
-
Make a ~2 cm paramedial submental incision
-
Location:
-
Parallel to the inferior border of the mandible
-
Approximately one finger breadth inferior to the mandibular border
-
-
-
Blunt Dissection
-
Pass a curved hemostat through:
-
Skin
-
Subcutaneous tissue
-
Platysma
-
Mylohyoid muscle
-
Submucosa
-
Oral mucosa
-
-
-
Intraoral Exit Point
-
Entry into the oral cavity occurs at the junction of attached lingual alveolar mucosa and free floor-of-mouth mucosa
-
Create a ~1 cm intraoral incision, parallel to the gingival margin
-
-
Exteriorization of the Tube
-
Deflate the cuff
-
Use a large curved hemostat or Kelly clamp
-
One prong stabilizes the cuff balloon
-
One prong stabilizes the tube
-
-
Gently pull the tube through the submental incision
-
-
Reconnection & Verification
-
Reattach the connector
-
Confirm ventilation
-
Anesthesia must confirm bilateral breath sounds to rule out mainstem intubation
-
-
Secure the Tube
-
Suture the tube to the skin using 1-0 or 2-0 silk sutures
-
Intraoperative Pearls
-
Always use an armored (reinforced) tube to prevent kinking
-
Make the incision slightly larger than you think you need
-
Ensure the cuff is fully deflated before exteriorization
-
Always reconfirm tube position after repositioning
-
Secure the tube firmly to prevent accidental displacement
Advantages Over Tracheostomy
-
Avoids tracheal injury
-
No long-term stoma or scar
-
Lower infection risk
-
Faster postoperative recovery
-
Easily reversible at the end of surgery
Conclusion
Submental intubation is a reliable, low-morbidity airway technique for complex maxillofacial cases where nasotracheal intubation is unsafe and tracheostomy is undesirable. Mastery of the paramedial technique allows surgeons to safely manage the airway while maintaining optimal surgical access and minimizing patient risk.
Board & Exam Pearls
-
Use armored ETT only
-
Paramedial incision avoids genioglossus, geniohyoid, digastric
-
Indicated in pan-facial trauma + CSF leak
-
Always deflate cuff before exteriorization
-
Confirm bilateral breath sounds