Airway Evaluation: Key Concepts for Safe Intubation and Anesthesia
By Dr. Paul Mirdamadi
A thorough airway evaluation is a critical component of safe anesthesia delivery. Proper positioning, accurate airway classification, and recognition of pediatric anatomic differences allow clinicians to anticipate difficulty, select appropriate equipment, and minimize complications during intubation.
This article reviews essential concepts in airway evaluation, including the sniffing position, Mallampati classification, Cormack–Lehane views, and pediatric airway considerations, along with practical formulas for endotracheal tube selection.
Sniffing Position
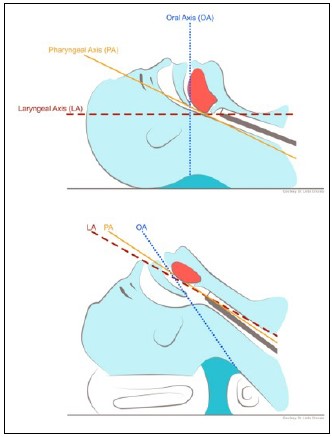
The sniffing position is the standard position for direct laryngoscopy and endotracheal intubation in adults. This position optimizes visualization of the glottis by physiologically aligning the three airway axes:
-
Oral axis
-
Pharyngeal axis
-
Laryngeal axis
It is achieved by flexing the neck at the cervical spine while extending the head at the atlanto-occipital joint. Proper positioning significantly improves the likelihood of successful laryngoscopy and reduces intubation difficulty.
Mallampati Classification
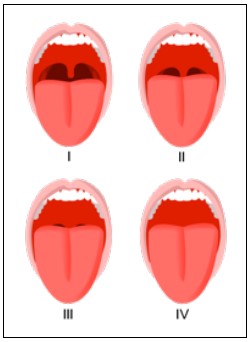
The Mallampati classification is a preoperative airway assessment tool used to estimate the difficulty of intubation based on oropharyngeal anatomy. It is evaluated with the patient sitting upright, mouth fully open, and tongue protruded.
-
Class I: Soft palate, uvula, and tonsillar pillars visible
-
Class II: Soft palate and uvula visible; tonsillar pillars not seen
-
Class III: Only the base of the uvula visible
-
Class IV: Only the tongue and hard palate visible
Higher Mallampati classes (III and IV) are associated with an increased risk of difficult intubation but should always be interpreted in combination with other airway findings.
Cormack–Lehane Laryngoscopic Views
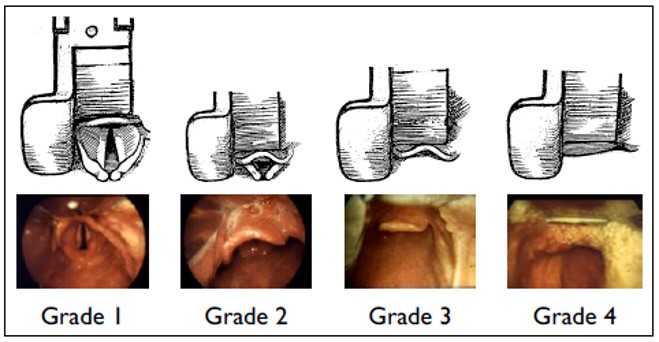
The Cormack–Lehane grading system describes the view obtained during direct laryngoscopy and correlates strongly with intubation difficulty.
-
Grade I: Full view of the glottis
-
Grade II: Only the posterior commissure of the glottis visible
-
Grade III: No glottic structures visible
-
Grade IV: Neither the glottis nor the corniculate cartilages visible
Grades III and IV are associated with difficult or failed intubation and often require adjuncts or alternative airway techniques.
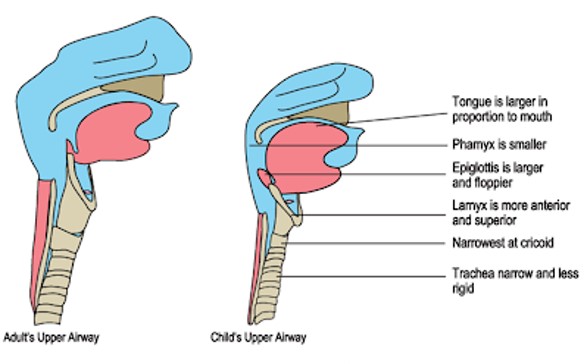
Pediatric Airway Considerations
Pediatric airways differ anatomically from adult airways and present unique challenges during intubation.
Key pediatric differences include:
-
A floppy, omega-shaped epiglottis that is more difficult to control
-
A more cephalad larynx, typically at C3–C4, compared to C4–C5 in adults
-
Vocal cords angled more caudally, rather than perpendicular to the airway
-
A proportionally larger tongue relative to oral cavity size
These factors require greater displacement of the tongue and mandible to visualize the vocal cords. As a result, straight laryngoscope blades (Miller blades) are more commonly used in infants and young children to directly lift the epiglottis.
Endotracheal Tube (ETT) Selection
Accurate ETT sizing is essential to avoid airway trauma, inadequate ventilation, or excessive leak.
ETT internal diameter (mm) can be estimated using:
-
(Age ÷ 4) + 4
-
Height (cm) ÷ 20
ETT depth at the lips:
-
Oral intubation: 3 × tube size (mm)
-
Nasal intubation: 4 × tube size (mm)
In children ≤ 8 years of age, uncuffed endotracheal tubes are traditionally recommended due to the funnel-shaped airway and narrow cricoid cartilage, although cuffed tubes may be used selectively with careful pressure monitoring.
Clinical Importance
Effective airway evaluation:
-
Reduces the risk of failed intubation
-
Improves patient safety during anesthesia
-
Guides equipment selection and backup planning
-
Is frequently tested on anesthesia and surgical board exams
Airway assessment should always be multifactorial, incorporating physical examination, patient history, and anticipated procedural needs.
Board and Exam Pearls
-
Sniffing position aligns oral, pharyngeal, and laryngeal axes
-
Mallampati predicts difficulty but is not diagnostic alone
-
Cormack–Lehane is an intraoperative grading system
-
Pediatric larynx is higher and more anterior
-
Use Miller blade in infants to lift the epiglottis
-
ETT size ≈ (age/4) + 4
Conclusion
A systematic airway evaluation is foundational to safe anesthesia practice. Understanding airway anatomy, classification systems, and age-specific differences allows clinicians to anticipate challenges and manage the airway confidently and effectively.